Scant evidence to support roll out of social prescribing policy internationally
. DOI: 10.1136/bmjopen-2022-062951")
There’s scant evidence to support the roll out of social prescribing policy internationally, concludes a review of the available evidence, published in the open access journal BMJ Open.
Social prescribing is a way of linking people with complex needs to non-medical support in their local community as part of a holistic approach to care. The non-medically qualified link worker model is the one most frequently used in the U.K.
The review found no consistent evidence that social prescribing improves social support, physical function, or reduces use of primary health services, and only limited evidence that it improves subjective assessment of personal health or quality of care received.
NHS England is funding link workers in primary care and recommends their use for people with one or more long term conditions, or who need support with their mental health, are living in deprived communities, or who have complex social problems.
Previous reviews of the evidence have mostly focused exclusively on U.K. practice and have included a broad range of studies without comparison groups. And social prescribing is a rapidly evolving field and gaining momentum, say the researchers.
In a bid to plug this knowledge gap, they set out to systematically review the evidence on effectiveness and costs of the link worker model of social prescribing internationally, and to establish the evidence, if any, on how well this approach works in people with several coexisting health conditions and who are living in deprived communities.
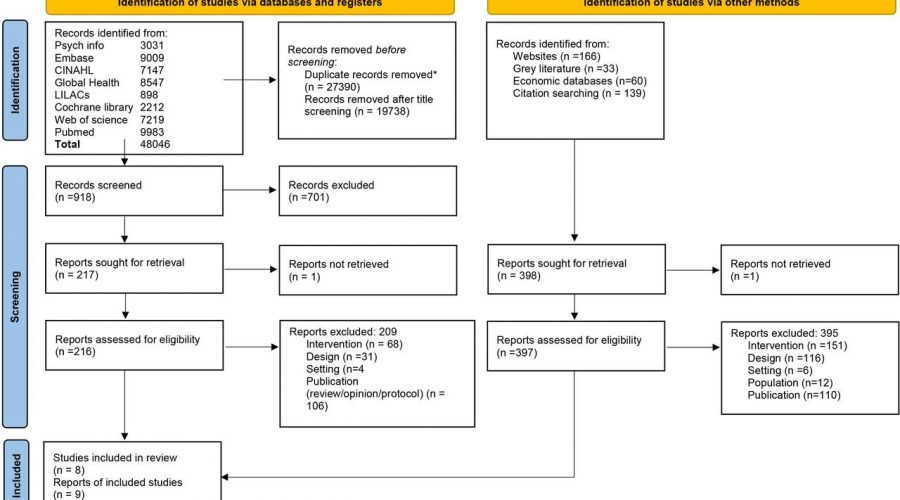
They searched 11 research databases for relevant comparative (controlled) clinical trials, as well as “gray literature,” such as government reports and conference proceedings, published up to July 2021.
The search generated eight studies, involving 6,500 people. Five were randomized controlled trials; three were controlled before and after studies; one reported the economic evaluation of an included trial. Four included people with several coexisting conditions and who were living in deprived communities. Three studies were from the U.S.; five were from the U.K.
The intervention periods ranged from one month to two years, with most lasting three to nine months. Few studies reported on link worker caseload or number of contacts.
Resources to which clients were signposted included counseling services, social and craft groups, exercise classes, addiction support services, and welfare and employment advice.
Four studies (2,186 participants) found that social prescribing made no difference to health-related quality of life. Of the four (1,924 participants) reporting mental health outcomes, three found no impact for social prescribing.
Of the four studies that reported a measure of physical activity and function, one found an improvement in functional health; two found no evidence of a difference in activities of daily living or physical activity; and one found a reduction in routine activities.
Of the four studies reporting on primary health care use, one reported a reduction in primary care attendance in the intervention group, but the comparison group was very different. Of the remainder, two found no evidence of a change in use, while one U.S.-based study found that attendance actually increased.
Two U.S. studies found that clients rated the quality of their care more highly and that social prescribing reduced hospital admissions for people with several co-existing conditions and who were socially isolated.
But none of the studies included in the review formally analyzed cost effectiveness. And while one study found that health care costs fell because of fewer referrals, these savings didn’t offset the costs of the intervention itself, prompting the study authors to conclude that social prescribing was more expensive than usual care.
The limited number of studies and the wide variations in study design, study participants, and interventions precluded a pooled data analysis of the results of the eight studies, so weakening the strength of the review findings, caution the researchers.
“Policy makers need to be aware that there is insufficient evidence to assess the effectiveness of social prescribing link workers and none on the cost-effectiveness, so the opportunity cost is unknown,” added to which there are no agreed outcomes or measures for social prescribing, highlight the researchers.
They conclude: “Our systematic review suggests that link workers providing social prescribing may have little or no impact on [health related quality of life], mental health or a range of patient-reported outcomes though they may improve self-rated health.
“For patients with multi morbidity in areas of deprivation, an intensive link worker intervention probably improves patients’ ratings of high-quality primary care and reduces hospitalizations, but these findings are based on two studies in the U.S. and require evaluation in other health systems.
Source: Read Full Article