Challenging assumptions on the economic costs of dementia
. DOI: 10.1002/alz.12619")
Increasingly severe cognitive, behavioral, or motor symptoms due to the dysfunction and death of the brain’s nerve cells are the hallmarks of the diseases that cause dementia. There is no cure and, therefore, patients with Alzheimer’s disease, vascular dementia, or other dementias have a growing need for care as the disease progresses. With populations around the world aging, the number of people experiencing dementia is increasing and so the associated global costs following diagnosis is assumed to be tending towards $2 trillion, thus creating major societal challenges and economic pressure to provide high quality care.
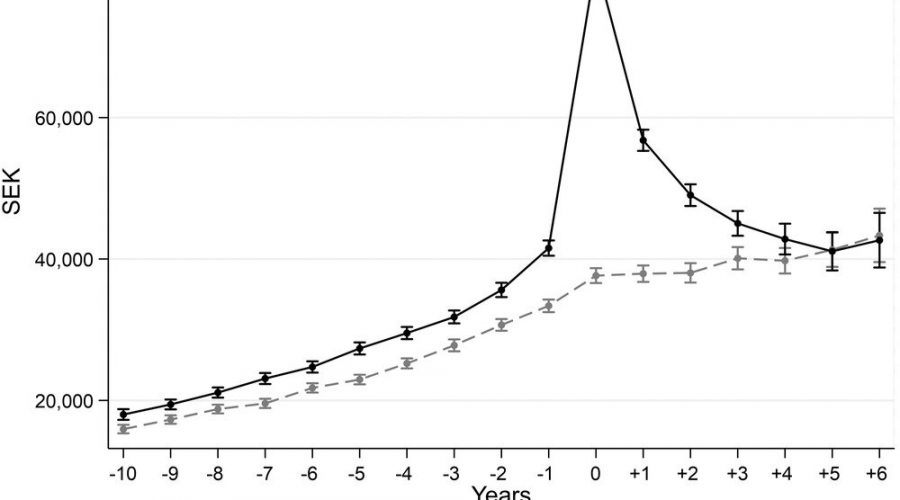
In this respect, researchers at the Global Brain Health Institute (GBHI) at Trinity College, undertook a new study in collaboration with the Health Economics Unit of Lund University in Sweden, which has revealed previously unknown aspects of how health care costs develop over the course of the disease. Curiously, health care costs were significantly higher as early as 10 years before dementia diagnosis. And, while care costs increased, and indeed doubled, at diagnosis, this new research challenges existing assumptions about the economic implications of dementia as a few years after diagnosis, costs drop to the same, or even lower, levels than in those without dementia. This raises real equity concerns for people living with dementia. For example, do people with dementia receive the health care they need as things get more difficult, or have our systems developed a tendency to displace the burden of care on others?
This register-based study, published in the journal Alzheimer’s & Dementia, the journal of the Alzheimer’s Association, examines the full population of people living with dementia in Region Skåne in southern Sweden. These 21,184 people were first identified as having a dementia diagnosis between 2010 and 2016. The research insights were made possible as individuals registered in Sweden’s national dementia registry can be linked to routinely collected healthcare data such as from primary healthcare, inpatient, and outpatient care. These data enabled the research team to examine individuals living with dementia over a 17-year period, including the year of diagnosis, 10 years before, and 6 years after diagnosis.
Dr. Dominic Trepél, Assistant Professor of Health Economics at the School of Medicine at Trinity and the Global Brain Health Institute (Trinity and UCSF), said: “Our results support the brain health hypothesis that policy should take a life-course view in reducing the risk of dementia and support the growing idea that policymakers should allocate resources to reduce dementia risk factors, in line with high-level recommendations from The Lancet Commission on Dementia Prevention, Intervention and Care.”
What is driving dementia health care costs?
The team is now undertaking further research, using state-of-the-art statistics methods, to explore what is driving the excess health care costs before diagnosis and why the marginal cost is lower in the subsequent years after diagnosis. For example, is the drop in health expenditure after diagnosis due to the initiation of treatments and social care provided by the municipalities, which substitutes for the need for health care? And if so, are costs being appropriately displaced onto social care, or onto families? And, could the initial increases in cost at diagnosis be related to difficulty in getting a definitive dementia diagnosis?
Source: Read Full Article