
Did the COVID lockdowns work? Heres what we know two years on

Since the UK first entered lockdown on March 23 2020, little in the pandemic has attracted so much attention and controversy as this decision to grind social and economic life to a halt. Was it the right thing to do?
Properly evaluating the effectiveness of any health-oriented treatment, be it a new medicine, vaccine or lockdown measure, involves comparing its introduction with a counterfactual situation where everything is the same except for what’s being tested. This is why medical trials have a control group, whose members are given a placebo and whose characteristics match the testing group as closely as possible.
Unfortunately, this isn’t possible for lockdowns. There are no directly equivalent parts of a country or the world that can act as true test and control groups, and so no possibility of a controlled trial. Instead, researchers must resort to other methods to try to measure lockdowns’ effects.
Mathematical models can be used to produce “what if” scenarios, where applying various different COVID control measures is simulated to estimate what would work best, essentially comparing the value of lockdown to other measures—or doing nothing at all. Such models are very useful and have been used throughout the pandemic.
However, they’ve also been heavily criticised for their pessimistic predictions about the impact of the virus. Their outputs depend on making assumptions and estimates, including about human behaviour, which is notoriously difficult to capture accurately.
An alternative is to use a data-driven method that doesn’t rely so strongly on the assumptions of models. For example, the “difference-in-difference” method compares outcomes from countries or regions that are similar in all respects except the implemented control measures. A common approach has been to compare data from US states that differed in the stringency, timing and extent of their control measures but otherwise share many characteristics.
But of course, this runs into our initial problem. While often similar, no two states aren’t directly comparable. And for other countries, like the UK, its even more difficult to find good pairings for comparison.
Imperfect assessments, clear results
Despite these difficulties, a lot of researchers have worked to try to analyse the impact of lockdowns. While accepting that no method of assessment is perfect, most published studies have found evidence to support lockdown measures being effective. They also point out that different actions achieved different things in different countries.
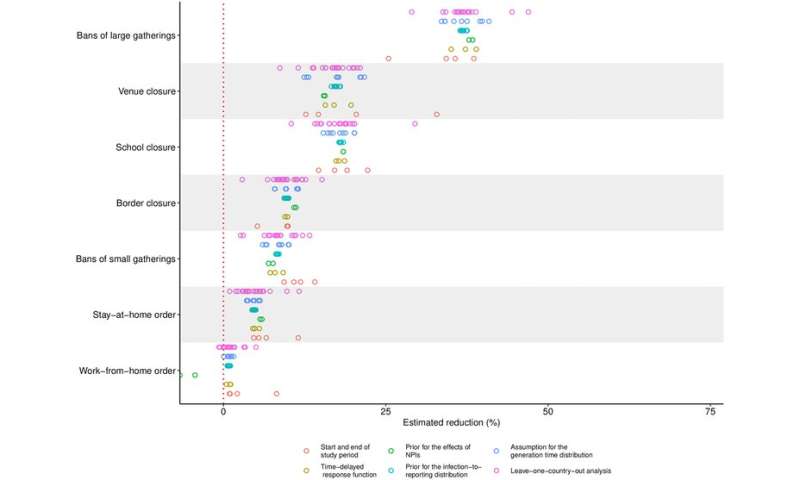
Limiting gatherings, closing businesses with high exposure rates, and closing schools and universities effectively reduced the spread and limited deaths. These places are associated with increased transmission rates and superspreader events.
But perhaps surprisingly, stay-at-home orders appear to have had only a modest effect in slowing transmission. This may, though, be down to people already limiting their activities voluntarily before being told to do so. Closing airports somewhat limits the disease impact, but land borders much less.
The danger of delaying
So, were lockdowns appropriate strategy, or should governments in future rely purely on voluntary isolation? Or is the best response to do nothing?
In evaluating the 2020 lockdowns, we need to remember that the decisions were taken with high uncertainty of what the consequences could be. It is easy to criticise the scientists and politicians in hindsight, but under the precautionary principle, the strongest possible measures should have been applied given the unknowns that were being faced.
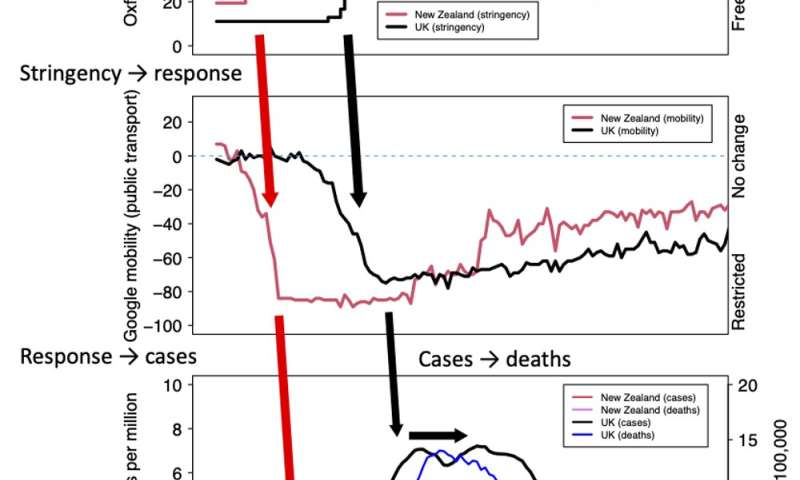
Despite substantial variability across countries, there’s little doubt that lockdowns successfully slowed COVID’s spread in spring 2020, reducing cases in the first wave. There’s enough evidence to show that countries and regions that quickly introduced substantial and multiple restrictions also had fewer cases and deaths. Compare New Zealand’s and the UK’s responses.
In both cases the introduction of lockdown regulations (first graph above) resulted in a rapid drop in mobility (second graph above). Reported cases peak soon after. Deaths in turn took another week or two to respond.
But New Zealand responded very quickly to its first reported case, with its lockdown introduced well before the first death in the country. Its resulting case numbers and deaths were low. In contrast, the UK delayed its lockdown response until almost two weeks after its first death.
Although British people reduced their mobility before lockdown was officially introduced, the virus had ample time to spread. The fact that delaying lockdown had such a large impact is further proof of its power to control the spread of the virus.
Lessons for the future
Should the world face another new pandemic disease, there are three lessons to keep in mind. Firstly, applying protective measures as early and hard as possible consistently led to better outcomes. Less stringent interventions risked increasing deaths; more severe responses lowered fatalities.
Plus, unless it’s possible to eliminate the virus in a region, measures will need to continue. This requires public acceptance and economic support, particularly in areas of high deprivation. And finally, for the greatest effect, different restrictions must be combined, including voluntary responses—such as social distancing—and test and trace. There’s no single silver bullet. Some measures might need maintaining, even after, for example, introducing vaccines.
Source: Read Full Article